The Doctor Will See You Now — On America’s Terms: What Africa Must Understand About the America First Global Health Strategy
Eighteen+ African nations have signed sweeping bilateral health agreements with the United States. The headline promise is billions of dollars in support for HIV, malaria, and tuberculosis. The fine print involves data sovereignty, pathogen sharing, and in at least one case, minerals.

Becon Format: Facts / ADC Analysis / The Counter Current / What Else Matters / Sovereign Solutions in Action
What We Know
On September 18, 2025, the United States State Department released the America First Global Health Strategy (AFGHS). In plain language, it is Washington's new framework for how America will spend its global health dollars — and what it expects in return. The strategy rests on three declared pillars: making America safer by stopping infectious disease outbreaks before they reach U.S. shores; making America stronger by replacing large NGO-driven aid with direct government-to-government bilateral agreements; and making America more prosperous by promoting American health innovation, technology companies, and private-sector interests in partner countries. The document is publicly available at state.gov, and every African policymaker who has not read it should do so before the end of the week.
The strategy followed the Trump administration's earlier dismantling of USAID and a near-70 per cent cut to annual global health spending, which left health programmes across the continent in acute crisis. The AFGHS is the replacement architecture. Instead of channelling money through multilateral institutions and large international NGOs, Washington wants direct, country-to-country deals — five-year Memorandums of Understanding that require each partner government to commit to increasing its own domestic health spending as U.S. assistance simultaneously declines over the same period. The stated goal is self-reliance. The structural effect is that Africa pays more for the same outcomes as American funding falls.
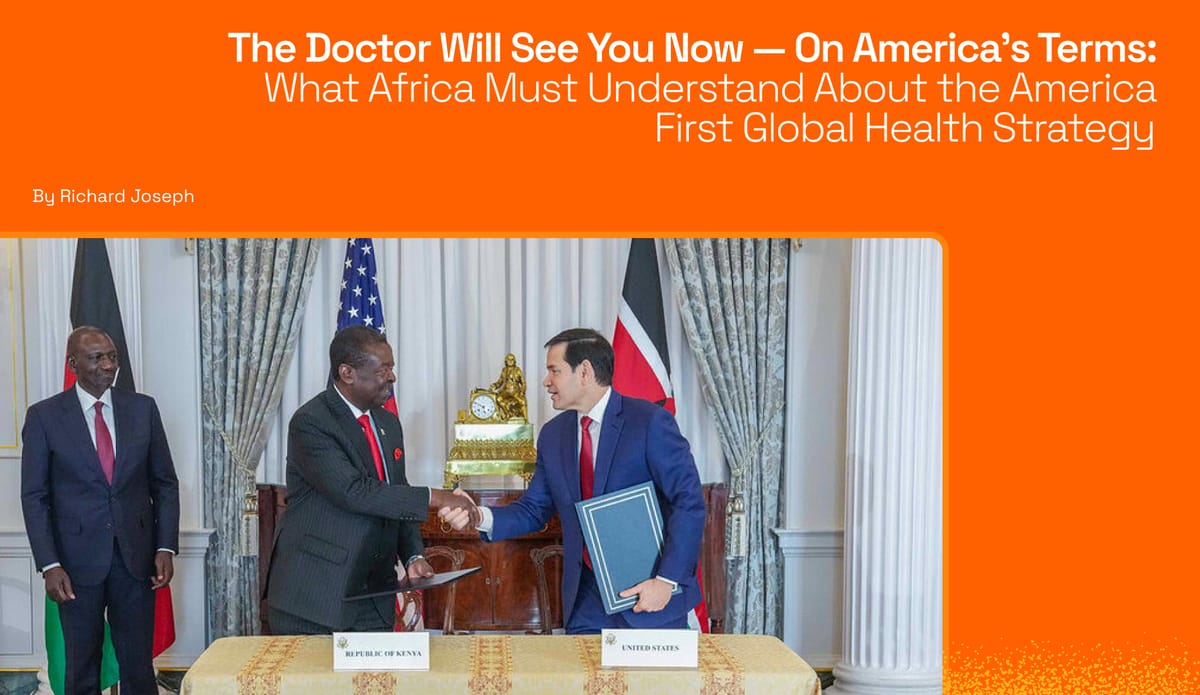
Between December 2025 and early 2026, the United States signed these agreements with fourteen African nations. Kenya was first, on December 4, 2025, in a ceremony attended by Secretary of State Marco Rubio and President William Ruto. The fourteen countries that have signed are: Kenya, Rwanda, Uganda, Liberia, Lesotho, Eswatini, Mozambique, Cameroon, Nigeria, Côte d’Ivoire, Malawi, Botswana, Madagascar, and Sierra Leone. Their agreements collectively represent billions of dollars in U.S. health commitments. Yet as the Centre for Global Development has documented, these MOUs represent an average 49 per cent reduction in annual U.S. health funding compared to what these same countries received in fiscal year 2024.
The Money: What Each Country Signed For
Nigeria signed the largest agreement — a five-year MOU worth $5.1 billion in total, with the United States committing nearly $2.1 billion and Nigeria pledging close to $3.0 billion in new domestic health expenditure. Ethiopia followed with a $1.466 billion U.S. commitment and $450 million in Ethiopian government co-investment, covering HIV/AIDS, tuberculosis, malaria, and maternal health. Uganda concluded an agreement worth approximately $2.3 billion, and Kenya's deal is valued at around $1.6 billion in U.S. funding over five years. Rwanda's agreement is comparatively smaller at $228 million. Botswana's deal involves $106 million in U.S. assistance against $381 million in Botswana's own co-investment — a ratio that tells you everything about whose health system is being built.
Every MOU contains six programmatic areas: health commodities, frontline health workers, data systems, disease surveillance and outbreak response, laboratory systems, and a flexible strategic assistance category. The agreements also include shared performance benchmarks with consequences for non-performance, including the termination of U.S. support if targets are not met. Importantly, of the fourteen MOUs signed, only three — Kenya's, Uganda's, and Liberia's — have been made publicly available. Citizens of the eleven other signatory countries cannot read what their governments agreed to on their behalf.
"Foreign assistance is not charity; it is designed to further the national interests of the United States. — Secretary of State Marco Rubio"
THE ADC PERSPECTIVE
What the Strategy Actually Does — and Who It Is For
The Data Question
At the heart of the AFGHS — and at the heart of every concern raised by governments, courts, and civil society across the continent — is data. Not health data as an abstraction, but the lived biological information of hundreds of millions of Africans: their viral loads, their pathogen exposures, their disease patterns, their genomic profiles. The strategy is explicit about its interest in this data. A model specimen-sharing agreement obtained by Health Policy Watch reveals that signatory countries agree to share specimen data with the United States within five days of receiving a request — and that the U.S. government can then share that specimen and related data with up to ten non-government American entities with the capacity to develop diagnostics and medical countermeasures. Those entities, in plain terms, are American pharmaceutical and biotech companies.
The question Africans are rightly asking is not paranoid — it is the same question any sovereign nation should ask before signing an agreement of this nature. If African health data is used to develop new vaccines, treatments, or diagnostics, will African nations receive equitable access to those products? The short answer, as currently written, is: there is no guarantee. Africa provides the raw biological material. American companies develop the innovations. And then, as we have already seen with HIV treatments including lencapavir, access is mediated by political considerations rather than public health needs. South Africa, which carries the world's largest HIV burden, was explicitly excluded from receiving lencapavir doses under the PEPFAR-Global Fund-Gilead initiative because of political tensions with Washington.

The worst that can happen if African countries sign away their complete health data without sufficient safeguards is not hypothetical — it is already visible in adjacent sectors. Health data from Africans has commercial value in pharmaceutical research, insurance modelling, and AI-driven diagnostics development. China recognised this and has codified data as a critical, high-value strategic national resource in its domestic legislation. African nations have not done this at scale. Until they do, every bilateral agreement that touches data creates an asymmetry that compounds over time: Africa generates the data, and American companies generate the profit.
Why This Strategy Is Focused Almost Exclusively on Africa
Of the 87 countries that received U.S. global health funding in fiscal year 2023, the ten largest recipients were all in Africa: DRC, Ethiopia, Kenya, Malawi, Mozambique, Nigeria, South Africa, Tanzania, Uganda, and Zambia. The African continent also reported more than 100 disease outbreaks in 2024 alone, according to the AFGHS document itself. From a purely epidemiological standpoint, the disease burden concentration in Africa explains the geographic focus. But the strategy is not purely epidemiological.
The AFGHS contains a section explicitly titled ‘Leveraging U.S. Global Health Leadership to Compete with China.’ One of its stated goals is to counter Chinese influence in the African region through health diplomacy. The disease surveillance networks, the laboratory capacity, the data systems — these are infrastructure investments that serve American geopolitical interests as much as African health interests. African countries are the terrain on which this strategic competition is being conducted. Countries outside Africa are largely absent from this framework, partly because of the disease burden concentration, and partly because — as the strategy is candid about — Africa represents the highest-risk zone for the kinds of infectious disease outbreaks that could reach American shores. Africa, in this framework, is simultaneously a patient and a perimeter.
The Reciprocity Problem
One of the most structurally important questions raised by community observers is also the simplest: if an African country were to draft an equivalent agreement — a Ghana, Kenya, Malawi, or Burkina Faso First Health Strategy, for instance — and asked the United States to share its citizens' health data as a condition of receiving African health cooperation, would Washington agree? The answer, plainly, is no. There is no reciprocal data-sharing obligation in any of the fourteen MOUs signed. The United States does not offer its epidemiological data in exchange. The surveillance flows in one direction. This asymmetry is not incidental to the design of the strategy — it is the design.
The Funding Reduction Hidden Inside the Partnership Language
Perhaps the most important fact to understand about the AFGHS — and the one most obscured by the headline dollar figures — is that annual U.S. health assistance will decline over the five-year period for every country that has signed. The Centre for Global Development's analysis is precise: the agreements represent an average 49 per cent reduction in annual U.S. health support compared to fiscal year 2024 levels. Nigeria's MOU, for all its $5.1 billion total figure, requires Nigeria to commit nearly $3 billion of its own money. Zambia, whose deal was due to be signed in November 2025, was offered $1.012 billion over five years — less than the $1.5 billion its Health Minister had publicly announced was agreed, and less than the $367 million Washington had committed to HIV services in Zambia alone the previous year.
The World Bank projects that government health spending in low-income and lower-middle-income countries will stagnate between now and 2030, with the combined effect of donor cuts meaning total health spending will fall in approximately 80 per cent of low-income countries. The AFGHS co-investment requirements were designed against an assumption of rising African state budgets. They are being implemented against a backdrop of fiscal stress. Countries that miss performance benchmarks lose U.S. support. There is no symmetrical consequence for the United States if it fails to deliver its committed funding.
THE HOLDOUTS
Zambia and Zimbabwe: When ‘No’ Is the Most Sovereign Word
On February 25, 2026, two significant decisions became public on the same day. Zimbabwe formally halted its bilateral health negotiations with the United States, rejecting a $367 million deal its government described as ‘clearly lopsided’ and incompatible with national sovereignty. In a letter dated December 23, 2025, Zimbabwe's Secretary for Foreign Affairs Albert Chimbindi communicated President Mnangagwa's instruction to the secretaries of finance and health: discontinue the negotiations entirely. The grounds were explicit: the agreement required Zimbabwe to share sensitive health and viral data without firm guarantees that Zimbabwe would benefit from any vaccines or treatments developed using that data; there was no reciprocal U.S. data-sharing commitment; and the arrangement was structurally inequitable in ways the President considered a compromise of Zimbabwe's sovereignty and independence.
On the same day, Zambia's government confirmed that it had pushed back on a draft MOU worth more than $1 billion, after revised drafts included provisions the Ministry of Health said ‘did not align with the position and interests of the government of Zambia.’ Reuters, which reviewed a leaked draft, reported that Zambia's data-sharing obligation would last ten years — twice the length of the five-year agreement itself. The broader deal was also linked, according to three independent sources, to a separate bilateral compact proposed by Secretary Rubio to President Hichilema in November 2025 that was tied to mining collaboration. Zambia is Africa's second-largest copper producer and holds significant reserves of cobalt, nickel, manganese, graphite, lithium, and rare-earth elements. The U.S. denied any formal linkage while simultaneously acknowledging a plan to ‘unlock a substantial grant package of U.S. support in exchange for collaboration in the mining sector.’
Asia Russell, Executive Director of Health GAP, described Zambia's proposed terms as ‘vastly worse than other deals’ and characterised the U.S. approach as ‘shameless exploitation.’ Julius Kachidza of Zambia's Civil Society Self-coordinating Mechanism described the dynamic as being ‘held hostage.’ The practical cost of Zimbabwe's decision is not abstract. Between 2018 and 2020, PEPFAR covered between 32 and 42 percent of Zimbabwe's HIV spending. The country's government contributed between 2 and 12 percent of its own HIV costs over the same period. For a health system that is dependent on external funding, walking away from any deal is a serious financial risk. Zimbabwe chose to walk away nonetheless, and that choice deserves to be understood and respected as a sovereign decision, not dismissed as recklessness.
Dr Jean Kaseya, Director-General of the Africa Centres for Disease Control and Prevention, acknowledged the continental tension directly: ‘There are huge concerns regarding data, regarding pathogen sharing. We want to own our data in Africa.’ He indicated the Africa CDC would support both Zambia and Zimbabwe in further negotiations, while also supporting the fourteen signatories in implementing their agreements. This is a continental institution attempting to hold two incompatible positions because the underlying fault line — between the immediate health funding needs of populations and the long-term sovereignty interests of states — is real and unresolved.
"We want to own our data in Africa. — Dr Jean Kaseya, Director-General, Africa CDC"
THE COUNTER-CURRENT: Room for Disagreement
The Case for Engaging — and Why It Is Not Unreasonable
The analysis above is deliberately direct. But context sovereignty requires acknowledging arguments on the other side — including the ones that carry genuine weight.
The most important counterargument is the epidemiological one. PEPFAR, operating under previous U.S. administrations, is estimated to have saved over 26 million lives globally and prevented 7.8 million HIV-positive births. For countries where HIV treatment is not domestically funded at scale — Ethiopia, Mozambique, Liberia, Sierra Leone — the prospect of losing U.S. support entirely is not a theoretical negotiating risk. It is a question of whether people living with HIV continue receiving antiretroviral therapy. The governments that signed these agreements were not naive. They were calculating severe fiscal constraints that their populations could not wait for ideal terms.
There is also a legitimate argument that the AFGHS push toward domestic co-investment and government ownership of health systems — however imperfectly structured — addresses a real failure of the previous aid model. For decades, large U.S.-funded NGOs functioned as the effective health service delivery system in many African countries, creating parallel infrastructure that often bypassed and weakened national health ministries. The AFGHS explicitly aims to end this model. If implemented well, this transition could strengthen African health sovereignty in the medium term. If implemented badly — which the compressed timeline and reduced funding make likely — it risks destroying institutional capacity built over twenty years.
Chatham House's analysis notes that preventing disease outbreaks is an area of genuine alignment between African and American interests. Disease surveillance, laboratory capacity, and outbreak response infrastructure built under these MOUs serve African populations regardless of the geopolitical context in which they were funded. Finally, one should not treat African governments that signed as passive victims without agency. Nigeria's co-investment commitment of $3 billion is the largest any country has made under the AFGHS framework. These are states making strategic calculations, not simply accepting dictation.
WHAT ELSE MATTERS
Kenyan Courts, the Accra Reset, and the Architecture Below the Surface
Kenya's story is not yet finished. Within a week of signing — the first country to do so — a Kenyan High Court suspended the agreement's implementation following two legal challenges: one by the Consumer Federation of Kenya and one by Senator Okiya Omtatah, both raising concerns about patient data privacy and the bypassing of Parliament. Kenya's courts are doing the democratic work that the negotiation process did not. This raises a question that applies to every signatory country: do governments have the constitutional right to share citizens' health data outside the jurisdiction of sovereignty without those citizens' explicit consent? In most African constitutional frameworks, the answer is unclear at best, and negative at worst. National courts are viable accountability mechanisms, even when parliamentary oversight has already been bypassed.
The AFGHS did not emerge into a vacuum. In August 2025 — a month before the strategy was released — Ghana's President John Dramani Mahama convened the Africa Health Sovereignty Summit, which endorsed the Accra Initiative: a declaration calling for a reconfigured global health order grounded in equity, national ownership, and sustainable financing. The Accra Reset, launched at the UN General Assembly in September 2025, built on this momentum. These are not fringe positions. They represent an emerging continental consensus about what fair health partnerships should look like — and they were articulated, publicly, before the first AFGHS MOU was signed. The question is whether they produce enforceable frameworks or remain as eloquent statements.
The technology dimension also demands attention. One of the first concrete investments under the AFGHS was a $150 million grant to Zipline International, an American autonomous delivery company, to expand drone delivery of medical commodities across Rwanda, Ghana, Nigeria, Kenya, and Côte d’Ivoire. The innovation is operationally valuable. But it means that critical African health supply chain infrastructure is owned and operated by an American company, dependent on American satellite-based technology, and subject to American commercial and political decisions. The investment serves African patients today. The ownership question will matter tomorrow.

SOLUTIONS IN ACTION
What African Policymakers and Citizens Can Do
The AFGHS is not a monolith. Its implementation will be shaped, in part, by how African governments, courts, civil society, and continental institutions respond. Zimbabwe and Zambia have demonstrated that the word ‘no’ is available at real cost. Kenya's courts have demonstrated that democratic institutions can impose scrutiny after the fact. What the continent now needs is scrutiny before the fact, and the institutional architecture to make that scrutiny effective and sustained.
The most urgent immediate action is transparency. Of the eighteen+ MOUs signed, only three are public. African citizens cannot evaluate what their governments agreed to on their behalf if the agreements are secret. Civil society organisations, parliamentarians, and journalists in signatory countries should be formally demanding the publication of every MOU. This is the baseline requirement of accountable governance, not a radical position. Beyond transparency, African governments should pursue the legislative codification of health data as a strategic national resource — drawing on China's legal framework as a model. Data protection frameworks that classify health data as sovereign national infrastructure give governments legal tools they currently lack, both in current negotiations and in future ones.
At the continental level, the African Union and Africa CDC have signalled willingness to help countries navigate these agreements. The Accra Initiative and the Accra Reset offer a platform for articulating a collective African position on health data sovereignty that could serve as the basis for renegotiating terms in countries where MOUs are not yet finalised. For countries that have already signed, Rwanda's model of using foreign investment to build domestic capacity with mandatory skills transfer requirements and Ethiopia's approach of using the MOU framework to preserve two decades of PEPFAR-built institutional continuity suggest that even imperfect agreements can yield real gains when governments engage strategically with implementation.
The most fundamental question raised by the AFGHS is one Africa must answer regardless of what Washington does: what is the continent's plan for financing its own health systems? The trajectory of declining U.S. support, rising co-investment requirements, and performance conditionality is not unique to American health diplomacy. It is the direction in which all global health aid is moving. The window to build domestic health financing systems, develop African pharmaceutical manufacturing capacity, and establish continental data governance frameworks is not unlimited. The AFGHS is, among other things, a deadline.
Winter Is Coming — But Africa Can Choose How to Meet It
There is nothing inherently wrong with America putting itself first. Every nation does, and honesty about that is preferable to the pretence that foreign aid has ever been purely charitable. The problem is not that the United States has national interests. The problem is that eighteen African governments — and potentially more to come, including Ghana — are signing agreements whose full terms are not available to their own citizens, whose data provisions extend well beyond the life of the agreements themselves, and whose financial architecture locks in a trajectory of declining external support against domestic spending commitments that may prove undeliverable.
Zimbabwe chose sovereignty over funding. Zambia chose to push back and demand revision. Kenya's courts stepped in after the government did not. These are the kinds of institutional responses that a continent serious about its own health security needs to normalise — not as anti-American reflexes, but as the standard due diligence that any rational, self-respecting state should apply before sharing the biological data of its citizens with a foreign government and its commercial partners for a decade.
The Accra Initiative, the Accra Reset, and the Africa Health Sovereignty Summit should not be merely poetic, as many African convergence and conferences are. It must become the raw material of a continental position — one that, if translated into enforceable frameworks, actual data protection legislation, and coordinated negotiating postures, could change the terms on which Africa engages with the next iteration of this conversation. Executing this translation is the real work, which will not happen in communiqués. It will happen in parliaments, in courtrooms, in ministries of health that refuse to sign documents they have not read, and in the spaces where African voices lead the analysis.
Winter is coming. The question is whether Africa builds the infrastructure to meet it on its own terms.
ADC Editorial Note
This analysis uses the ADC Beacon Format, which separates verified facts from editorial analysis, preserves space for legitimate disagreement, and closes with documented examples of African-led solutions. All MOU financial figures are drawn from U.S. State Department press releases (state.gov) and U.S. Embassy country statements, cross-verified against the KFF Global Health MOU Tracker (kff.org, updated February 2026) and Centre for Global Development analysis (cgdev.org). Corrections and community expert responses are welcomed via blog.discoursechannel.com.
© 2026 Africa Discourse Channel. Context Sovereign Journalism.